Now that we understand the business requirements, we need to check if the current Data Architecture supports them.
If you’re wondering what to assess in our data architecture and what the current setup looks like, check the business case description.
· Assessing against short-term requirements ∘ Initial alignment approach · Medium-term requirements and long-term vision · Step-by-step conversion ∘ Agility requires some foresight ∘ Build your business process and information model ∘ Holistically challenge your architecture ∘ Decouple and evolve
Assessing against short-term requirements
Let’s recap the short-term requirements:
- Immediate feedback with automated compliance monitors: Providing timely feedback to staff on compliance to reinforce hand hygiene practices effectively. Calculate the compliance rates in near real time and show them on ward monitors using a simple traffic light visualization.
- Device availability and maintenance: Ensuring dispensers are always functional, with near real-time tracking for refills to avoid compliance failures due to empty dispensers.
The current weekly batch ETL process is obviously not able to deliver immediate feedback.
However, we could try to reduce the batch runtime as much as possible and loop it continuously. For near real-time feedback, we would also need to run the query continuously to get the latest compliance rate report.
Both of these technical requirements are challenging. The weekly batch process from the HIS handles large data volumes and can’t be adjusted to run in seconds. Continuous monitoring would also put a heavy load on the data warehouse if we keep the current model, which is optimized for tracking history.
Before we dig deeper to solve this, let’s also examine the second requirement.
The smart dispenser can be loaded with bottles of various sizes, tracked in the Dispenser Master Data. To calculate the current fill level, we subtract the total amount dispensed from the initial volume. Each time the bottle is replaced, the fill level should reset to the initial volume. To support this, the dispenser manufacturer has announced two new events to be implemented in a future release:
- The dispenser will automatically track its fill level and send a refill warning when it reaches a configurable low point. This threshold is based on the estimated time until the bottle is empty (remaining time to failure).
- When the dispenser’s bottle is replaced, it will send a bottle exchange event.
However, these improved devices won’t be available for about 12 months. As a workaround, the current ETL process needs to be updated to perform the required calculations and generate the events.
A new report is needed based on these events to inform support staff about dispensers requiring timely bottle replacement. In medium-sized hospitals with 200–500 dispensers, intensive care units use about two 1-liter bottles of disinfectant per month. This means around 19 dispensers need refilling in the support staff’s weekly exchange plan.
Since dispenser usage varies widely across wards, the locations needing bottle replacements are spread throughout the hospital. Support staff would like to receive the bottle exchange list organized in an optimal route through the building.
Initial alignment approach
Following the principle "Never change a running system," we could try to reuse as many components as possible to minimize changes.
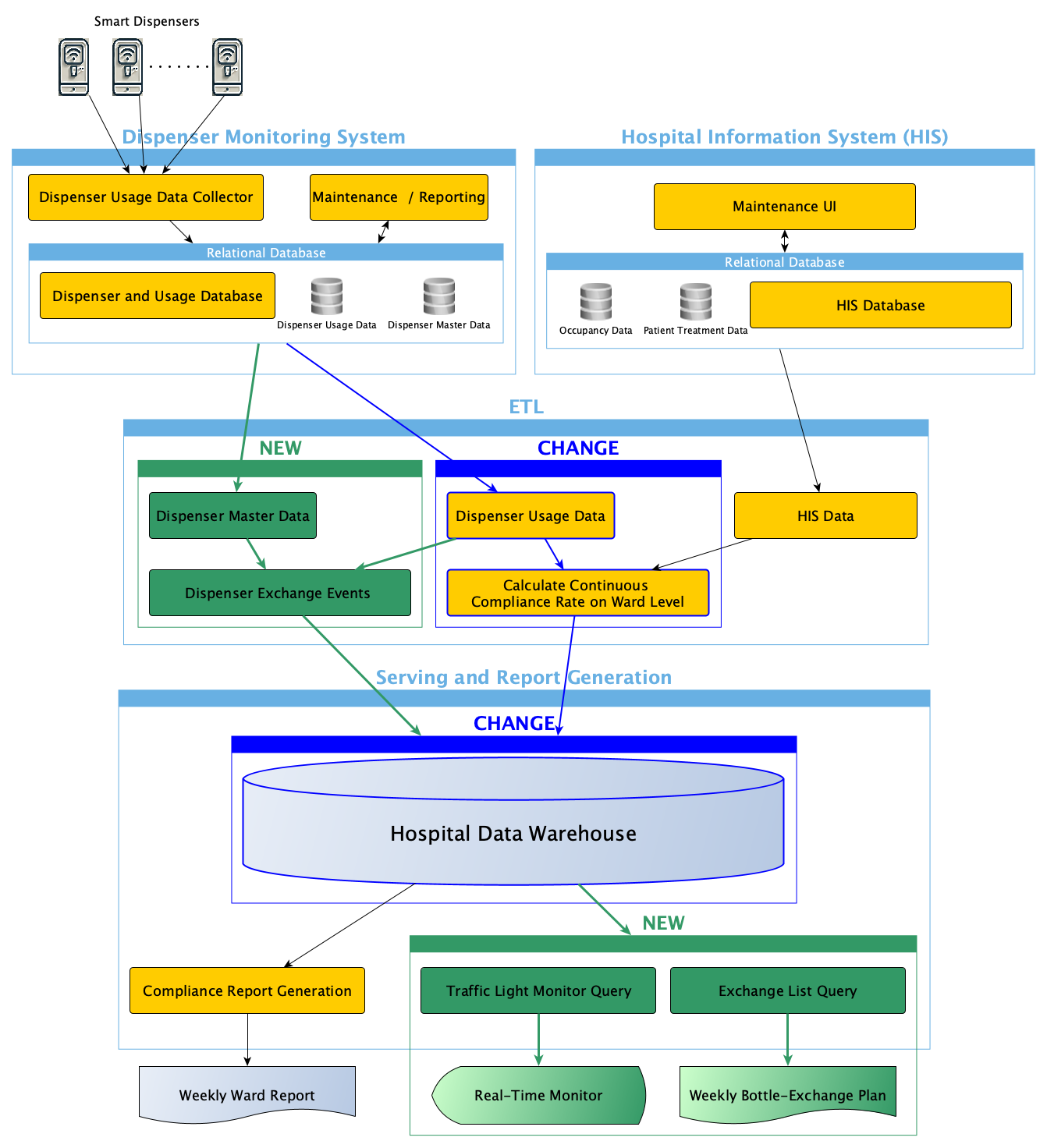
We would have to build NEW components (in green) and CHANGE existing components (in dark blue) to support the new requirements.
We know the batch needs to be replaced with stream processing for near real-time feedback. We consider using Change Data Capture (CDC)a technology to get updates on dispenser usage from the internal relational database. However, tests on the Dispenser Monitoring System showed that the Dispenser Usage Data Collector only updates the database every 5 minutes. To keep things simple, we decide to reschedule the weekly batch extraction process to sync with the monitoring system’s 5-minute update cycle.
By reducing the batch runtime and continuously looping over it, we effectively create a microbatch that supports stream processing. For more details, see my article on how to unify batch and stream processing.
Reducing the runtime of the HIS Data ETL batch process is a major challenge due to the large amount of data involved. We could decouple patient and occupancy data from the rest of the HIS data, but the HIS database extraction process is a complex, long-neglected COBOL program that no one dares to modify. The extraction logic is buried deep within the COBOL monolith, and there is limited knowledge of the source systems. Therefore, we consider implementing near real-time extraction of patient and occupancy data from HIS as "not feasible."
Instead, we plan to adjust the Compliance Rate Calculation to allow near real-time Dispenser Usage Data to be combined with the still-weekly updated HIS data. After discussing this with the hygiene specialists, we agree that the low rates of change in patient treatment and occupancy suggest the situation will remain fairly stable throughout the week.
The Continuous Compliance Rate On Ward Level will be stored in a real-time partition associated to the ward entity of the data warehouse. It will support short runtimes of the new Traffic Light Monitor Query that is scheduled as successor to the respective ETL batch process.
Consequently, the monitor will be updated every 5 minutes, which seems close enough to near real-time. The new Exchange List Query will be scheduled weekly to create the Weekly Bottle-Exchange Plan to be sent by email to the support staff.
We feel confident that this will adequately address the short-term requirements.
Medium-term requirements and long-term vision
However, before we start sprinting ahead with the short-term solution, we should also examine the medium and long-term vision. Let’s recap the identified requirements:
- Granular data insights: Moving beyond aggregate reports to gain insight into compliance at more specific levels (e.g., by shift or even person).
- Actionable alerts for non-compliance: Leveraging historical data with near real-time extended monitoring data to enable systems to notify staff immediately of missed hygiene actions, ideally personalized by healthcare worker.
- Personalized compliance dashboards: Creating personalized dashboards that show each worker’s compliance history, improvement opportunities, and benchmarks.
- Integration with smart wearables: Utilizing wearable technology to give real-time and discrete feedback directly to healthcare workers, supporting compliance at the point of care.
These long-term visions highlight the need to significantly improve real-time processing capabilities. They also emphasize the importance of processing data at a more granular level and using intelligent processing to derive individualized insights. Processing personalized information raises security concerns that must be properly addressed as well. Finally, we need to seamlessly integrate advanced monitoring devices and smart wearables to receive personalized information in a secure, discreet, and timely manner.
That leads to a whole chain of additional challenges for our current architecture.
But it’s not only the requirements of the hygiene monitoring that are challenging; the hospital is also about to be taken over by a large private hospital operator.
This means the current HIS must be integrated into a larger system that will cover 30 hospitals. The goal is to extend the advanced monitoring functionality for hygiene dispensers so that other hospitals in the new operator’s network can also benefit. As a long-term vision, they want the monitoring functionality to be seamlessly integrated into their global HIS.
Another challenge is planning for the announced innovations from the dispenser manufacturer. Through ongoing discussions about remaining time to failure, refill warnings, and bottle exchange events, we know the manufacturer is open to enabling real-time streaming for Dispenser Usage Data. This would allow data to be sent directly to consumers, bypassing the current 5-minute batch process through the relational database.
Step-by-step conversion
We want to counter the enormous challenges facing our architecture with a gradual transformation.
Since we’ve learned that working agile is beneficial, we want to start with the initial idea and then refine the system in subsequent steps.
But is this really agile working?
Agility requires some foresight
What I often encounter is that people equate "acting in small incremental steps" with working agile. While it’s true that we want to evolve our architecture progressively, each step should aim at the long-term target.
If we constrain our evolution to what the current IT architecture can deliver, we might not be moving toward what is truly needed.
When we developed our initial alignment, we just reasoned on how to implement the first step within the existing architecture’s constraints. However, this approach narrows our view to what’s ‘feasible’ within the current setup.
So, let’s try the opposite and clearly address what’s needed including the long-term requirements. Only then we can target the next steps to move the architecture in the right direction.
For architecture decisions, we don’t need to detail every aspect of the business processes using standards like Business Process Model and Notation (BPMN). We just need a high-level understanding of the process and information flow.
But what’s the right level of detail that allows us to make evolutionary architecture decisions?
Build your business process and information model
Let’s start very high to find out about the right level.
In part 3 of my series on Challenges and Solutions in Data Mesh I have outlined an approach based on modeling patterns to model an ontology or enterprise data model. Let’s apply this approach to our example.
Note: We can’t create a complete ontology for the healthcare industry in this article. However, we can apply this approach to the small sub-topic relevant to our example.
Let’s identify the obvious modeling patterns relevant for our example:
Party & Role: The parties acting in our healthcare example include patients, medical device suppliers, healthcare professionals (doctors, nurses, hygiene specialists, etc.), the hospital operator, support staff and the hospital as an organizational unit.
Location: The hospital building address, patient rooms, floors, laboratories, operating rooms, etc.
Ressource / Asset: The hospital as a building, medical devices like our intelligent dispensers, etc.
Document: All kinds of files representing patient information like diagnosis, written agreements, treatment plans, etc.
Event: We have identified dispenser-related events, such as bottle exchange and refill warnings, as well as healthcare practitioner-related events, like an identified hand hygiene opportunity or moment.
Task: From the doctor’s patient treatment plan, we can directly derive procedures or activities that healthcare workers need to perform. Monitoring these procedures is one of the many information requirements for delivering healthcare services.
The following high-level modeling patterns my not be as obvious for the healthcare setup in our example at first sight:
Product: Although we might not think of hospitals of being product-oriented, they certainly provide services like diagnoses or patient treatments. If pharmaceuticals, supplies, and medical equipment are offered, we even can talk about typical products. A better overall term would probably be a "health care offering".
Agreement: Not only agreements between provider networks and supplier agreements for the purchase of medical products and medicines but also agreements between patients and doctors.
Account: Our use case is mainly concerned with upholding best hygiene practices by closely monitoring and educating staff. We just don’t focus on accounting aspects here. However, accounting in general as well as claims management and payment settlement are very important healthcare business processes. A large part of the Hospital Information System (HIS) therefore deals with accounting.
Let’s visualize our use case with this high-level modeling patterns and their relationships.
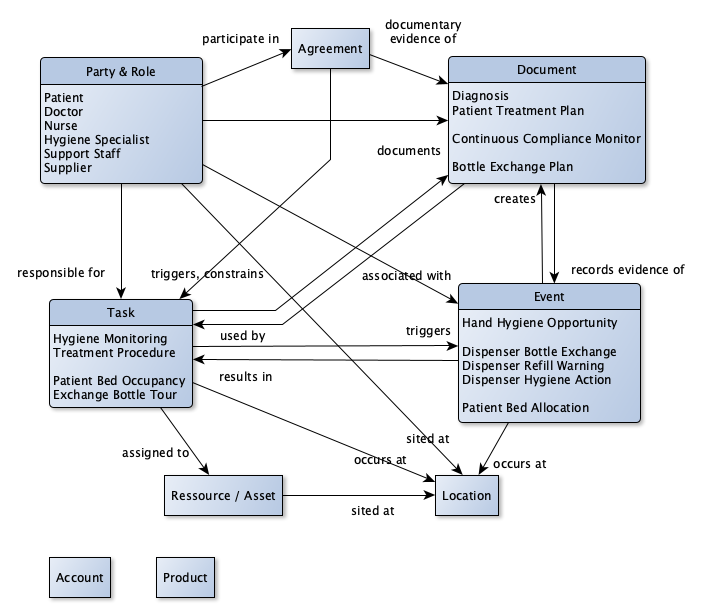
What does this buy us?
With this high-level model we can identify ‘hygiene monitoring’ as an overall business process to observe patient care and take appropriate action so that infections associated with care are prevented in the best possible way.
We recognize ‘patient management’ as an overall process to manage and track all the patient care activities related to the healthcare plan prepared by the doctors.
We recognize ‘hospital management’ that organizes assets like hospital buildings with patient bedrooms as well as all medical devices and instrumentation inside. Patients and staff occupy and use these assets over time and this usage needs to be managed.
Let’s describe some of the processes:
- A Doctor documents the Diagnosis derived from the examination of the Patient
- A Doctor discusses the derived Diagnosis with the Patient and documents everything that has been agreed with the Patient about the recommended treatment in a Patient Treatment Plan.
- The Agreement on the treatment triggers the Treatment Procedure and reflects the responsibility of the Doctor and Nurses for the patient’s treatment.
- A Nurse responsible for Patient Bed Occupancy will assign a patient bed at the ward, which triggers a Patient Bed Allocation.
- A Nurse responsible for the patient’s treatment takes a blood sample from the patient and triggers several Hand Hygiene Opportunities and Dispenser Hygiene Actions detected by Hygiene Monitoring.
- The Hygiene Monitoring calculates compliance from Dispenser Hygiene Action, Hand Hygiene Opportunity, and Patient Bed Allocation information and documents it for the Continuous Compliance Monitor.
- During the week ongoing Dispenser Hygiene Actions cause the Hygiene Monitoring to trigger Dispenser Refill Warnings.
- A Hygiene Specialist responsible for the Hygiene Monitoring compiles a weekly Bottle Exchange Plan from accumulated Dispenser Refill Warnings.
- Support Staff responsible for the weekly Exchange Bottle Tour receives the Bottle Exchange Plan and triggers Dispenser Bottle Exchange events when replacing empty bottles for the affected dispensers.
- and so on …
This way we get an overall functional view of our business. The view is completely independent of the architectural style we’ll choose to actually implement the business requirements.
A high-level business process and information model is therefore a perfect artifact to discuss any use case with healthcare practitioners.
Holistically challenge your architecture
With such a thorough understanding of our business, we can challenge our architecture more holistically. Everything we already understand and know today can and should be used to drive our next step toward the target architecture.
Let’s examine why our initial architecture approach falls short to properly support all identified requirements:
- Near real-time processing is only partly addressed
A traditional data warehouse architecture is not the ideal architectural approach for near real-time processing. In our example, the long-running HIS data extraction process is a batch-oriented monolith that cannot be tuned to support low-latency requirements.
We can split the monolith into independent extraction processes, but to really enable all involved applications for near real-time processing, we need to rethink the way we share data across applications.
As data engineers, we should create abstractions that relieve the application developer from low-level data processing decisions. They should neither have to reason about whether batch or stream processing style needs to be chosen nor need to know how to actually implement this technically.
If we allow the application developers to implement the required business logic independent of these technical data details, it would greatly simplify their job.
You can get more details on how to practically implement this in my article on unifying batch and stream processing.
- The initial alignment is driven by technology, not by business
Business requirements should drive the IT architecture decisions. If we turn a blind eye and soften the requirements to such an extent that it becomes ‘feasible’, we allow technology to drive the process.
The discussion with the hygiene specialists about the low rates of change in patient treatment and occupancy are such a softening of requirements. We know that there will be situations where the state will change during the week, but we accept the assumption of stability to keep the current IT architecture.
Even if we won’t be able to immediately change the complete architecture, we should take steps into the right direction. Even if we cannot enable all applications at once to support near real-time processing, we should take action to create support for it.
- Smart devices, standard operational systems (HIS) and advanced monitoring need to be seamlessly integrated
The long-term vision is to seamlessly integrate the monitoring functionality with available HIS features. This includes the integration of various new (sub-)systems and new technical devices that are essential for operating the hospital.
With an architecture that focuses one-sidedly on analytical processing, we cannot adequately address these cross-cutting needs. We need to find ways to enable flexible data flow between all future participants in the system. Every application or system component requires to be connected to our mesh of data without having to change the component itself.
Overall, we can state that the initial architecture change plan won’t be a targeted step towards such a flexible integration approach.
Decouple and evolve
To ensure that each and every step is effective in moving towards our target architecture, we need a balanced decoupling of our current architecture components.
Universal data supply therefore defines the abstraction data as a product for the exchange of data between applications of any kind. To enable current applications to create data as a product without having to completely redesign them, we use data agents to (re-)direct data flow from the application to the mesh.
Modern Data And Application Engineering Breaks the Loss of Business Context
By using these abstractions, any application can also become near real-time capable. Because it doesn’t matter if the application is part of the operational or the analytical plane, the intended integration of the operational HIS with hygiene monitoring components is significantly simplified.
Let’s examine how the decoupling helps, for instance, to integrate the current data warehouse to the mesh.
The data warehouse can be redefined to act like one among many applications in the mesh. We can, for instance, re-design the ETL component Continuous Compliance Rate on Ward Level as an independent application producing the data as a product abstraction. If we don’t want or can’t touch the ETL logic itself, we can instead use the data agent abstraction to transform data to the target structure.
We can do the same for Dispenser Exchange Events or any other ETL or query / reporting component identified. The COBOL monolith HIS Data can be decoupled by implementing a data agent that separates the data products HIS occupancy data and HIS patient data. This allows to evolve the data delivering components completely independent of the consumers.
Whenever the dispenser vendor is ready to deliver advanced functionalities to directly create the required exchange events, we would just have to change the Dispenser Exchange Events component. Either the vendor can deliver the data as a product abstraction directly, or we can convert the dispenser’s proprietary data output by adapting Dispenser Exchange Event data agent and logic.
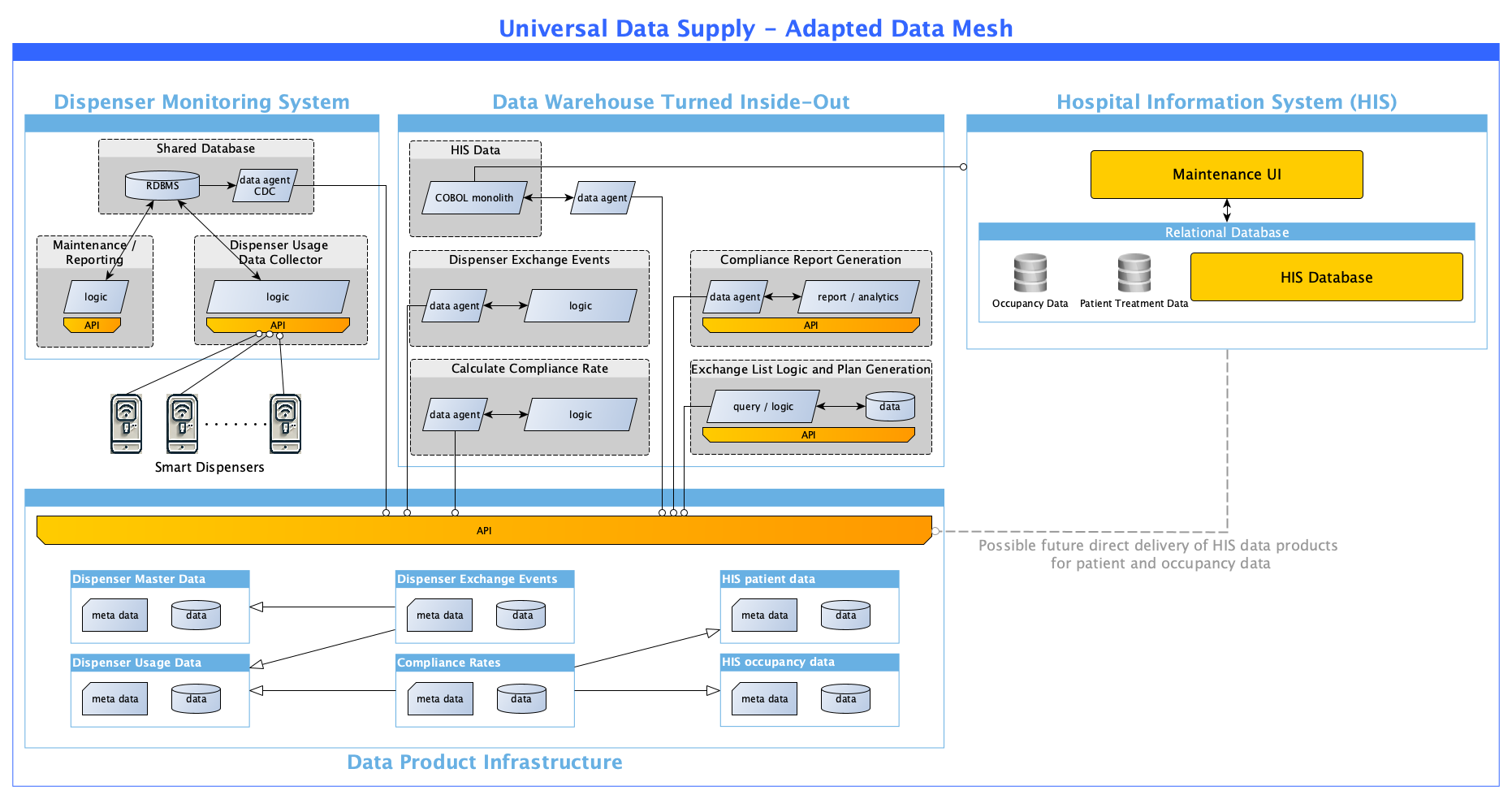
Whenever we are able to directly create HIS patient data or HIS occupancy data from the HIS, we can partly or completely decommission the HIS Data component without affecting the rest of the system.
We need to assess our architecture holistically, considering all known business requirements. A technology-constrained approach can lead to intermediate steps that are not geared towards what’s needed but just towards what seems feasible.
Dive deep into your business and derive technology-agnostic processes and information models. These models will foster your business understanding and at the same time allow your business to drive your architecture.
In subsequent steps, we will look at more technical details on how to design data as a product and data agents based on these ideas. Stay tuned for more insights!